
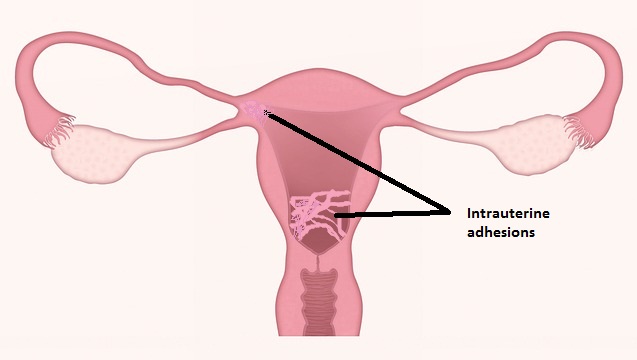
Asherman syndrome
Partial or complete damage of the uterine cavity due to the presence of permanent adhesions in the intrauterine lining is clinically termed as Asherman syndrome.
The traumatic injury in the endometrial basalis layer develops after curettage on the endometrial lining is the primary cause of Asherman syndrome.
In 1894, Heinrich Fritsch had first described this syndrome. Later Joseph G. Asherman explained the symptoms and pathology of this condition.
Women with Asherman syndrome may have amenorrhea (the absence of menstruation) along with other genital disorders like oligomenorrhea (infrequent menstruation), dysmenorrhea (painful menstruation), recurrent miscarriages and infertility.
Incomplete abortion, postpartum hemorrhage, and voluntary abortion are often required repeated application of curettage, which leads to traumatic injury in endometrial.
Resultant of this leads to the development of Asherman syndrome.
Apart from these, diagnostic curettage, hysterotomy, myomectomy, cesarean section, and tuberculosis are other contributory conditions responsible for Asherman syndrome development.
Hysteroscopy is the most reliable method for the detection of Asherman syndrome.
It allows direct visualization of the uterus.
Sonohysterography, hysterosalpingogram, and magnetic resonance imaging are the other methods have applied to detect this condition.
Hysteroscopic adhesiolysis is recommended to treat intrauterine adhesions.
Asherman syndrome associated with Pregnancy Complications
Women with Asherman syndrome have reported several obstetric complications, such as miscarriages, abnormal placentation, cervical incompetence, intrauterine growth retardation, premature birth, uterine rupture, and preeclampsia.
Asherman syndrome associated abnormality in the uterine endometrium.
The damaged uterine cavity may cause cervical or ectopic tubal pregnancies.
Clinical investigators also found serious complications in pregnancy including placenta previa (partial or complete uterine neck blockage by the placenta which restricts normal delivery), retained placenta, fetal death, and postpartum hemorrhage.
The complication depends upon the stages of Asherman syndrome.
Asherman syndrome may be mild, moderate and severe.
The stages of Asherman syndrome depend upon the degree of intrauterine adhesions.
The uterine growth during pregnancy is affected by the degree of intrauterine adhesions.
Close monitoring of an obstetrician is essential during the gestational period for women who had the previous history of Asherman syndrome.
Asherman syndrome associated with low birth weight
A recent retrospective study findings published in 2018 have reported that women with Asherman syndrome have a direct association with giving birth of a child with low birth weight in comparison with women who have a normal intrauterine cavity.
This study report has shown that 35.7% of preterm delivery occurs in women with Asherman syndrome.
However, the chances of delivery occurs in women with Asherman syndrome can vary and the range is lies between 17.9% and 50%.
The spontaneous conception rate with this syndrome is more than fifty percent.
Researchers have expected that the defective placentation in pregnant women with Asherman syndrome is a cause of intrauterine growth retardation.
This may occur because of the history of Asherman syndrome associated with endometrium damage.
Resultant of this can cause poor blood perfusion in the placental tissue because of the reduced supply of blood in the uterus and placenta.
Read Also: Pregnancy Planning Guide
Reference: NCBI

Ravi Sharma is a self-motivated, successful entrepreneur and has a solid experience in the fertility segment. and he is the director at ARTbaby Global (ARThealthcare). He is a pharmacy graduate with post-graduation in business administration and has 14 years of rich experience in the field of infertility segment. He loves to write about IVF, Surrogacy, and other ART (assisted reproductive technology) news, issues, and updates. He is a Pharmacy graduate (B. Pharm) and M.B.A (marketing).
His most recent success includes the successful launch of the medical tourism company, ARTbaby, which offers treatment options for infertility, egg donation, and surrogacy. He likes spending time with his family and writing about various aspects of IVF surrogacy and donating eggs.